|
Dr. Rana Tahir Naveed Assistant Professor University of Education E-mail:- ranatahir28@hotmail.com |
Ahmad Mohmad Albassami University Putra Malaysia (UPM) E-mail:- albassami9500@gmail.com |
Naveed Ahmad Faculty of Management Sciences Lahore Leads University, Pakistan E-mail:- naveeddgk2010@gmail.com |
Mahsa Moshfegyan Lecturer Salahadin University-Erbil E-mail:- m.mahsa@live.com |
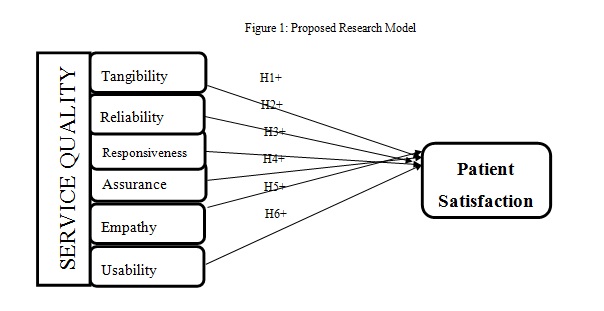
This study aims at investigating the modified SERVQUAL Model with sixth dimension of usability and its relation with patient satisfaction in private healthcare sector of Pakistan. To represent Private Healthcare sector, three large hospitals Iqra Hospital, Arif Memorial hospital and Hameed Latif were chosen. A total of 348 questionnaires were distributed among in-patients of these hospitals randomly and 261 fully filled questionnaires were received. Different statistical tools like descriptive statistics, Factor analysis, Correlation analysis and regression analysis were performed on SPSS software. The results of study showed that all six dimensions of SERVQUAL model like, Responsiveness, reliability, Empathy, Assurance, Tangibility and usability were significant predictors of Patient satisfaction in private healthcare sector of Pakistan but Responsiveness factor was the most dominant in this regard. The present study will help top management and policy makers of healthcare sector to craft better strategies for patient satisfaction through modified SERVQUAL model.
Keywords: Responsiveness, Reliability, Empathy, Assurance, Tangibility, Usability, Patient satisfaction
Presently every business sector is facing different challenges including survival and success issues and ever increasing competition further adds to these difficulties for business organizations. Service sector is also growing with a fast pace during recent decades and concern for quality in service is an important issue in present business scenario ( Ahmady et al., 2015 ). Quality is something that is really hard to imitate and for this reason quality is a crucial factor to earn favorable positioning (Ameryoun et al., 2017). Similarly in a research, Al-Borie & Sheikh Damanhouri (2013 ) highlighted the importance of service quality as they acknowledged it a key factor for successful business strategy especially those businesses that involve high client involvement like medical or financial services. ( Ali, Hussain, & Omar, 2016 )
Healthcare industry is one of the most rapidly growing industry and there are different factors responsible for this rapid growth in health care sector for example environmental changes, competitive pressures, alternate healthcare mechanism, new roles and regulations imposed by governments to improve healthcare facilities, access of patients to information, cost structures and many others contributed in this regard. So, many healthcare service providers realized that patient satisfaction is a key factor for long run success of a hospital. Hence patient satisfaction is considered to be a desired outcome for any hospital or healthcare service provider ( Madan & Goel, 2015 ). Patient satisfaction is an important profitable competitive strategy and different studies (for example, Yesilada & Direktör, 2010 ) have shown people are more concerned about those organizations which provide high standards of care and attempt to satisfy their customer in a better way. Mthethwa & Chabikuli ( 2016 ) argued in their research study that hospitals with better image of patient satisfaction grab better market share and survive in competition.
Similarly, patients of today are more informative and educated about healthcare service as compared to past. Due to their information and knowledge they carefully chose a hospital after observing different standards of healthcare according to their needs. So availability of information is a crucial factor due to which patients are much sensitive about delivery of healthcare services and facilities. Buyers of healthcare services are not trusting on doctors as heavily as was the case in past, rather they give weight to the opinion of previous patient’s experience at a certain hospital ( Dagger, Sweeney, & Johnson, 2007 ; Lee, & Kang, 2012 ). According to Panchapakesan, Sai, & Rajendran, (2015 ) it is not the issue whether patient is right or wrong, the issue is how a patient felt during his or her stay at a particular hospital. Healthcare service providers failing this understanding may invite trouble for their hospitals.
It goes without saying that patients’ satisfaction is a key factor in patients’ decision making while choosing a specific hospital. There are several general characteristics for patient satisfaction such as demographic, socioeconomic and general health status. Besides these general characteristics, patient satisfaction is also decided by the delivery of healthcare services from a hospital for example experience of doctor and healthcare delivery environment ( Madan & Goel, 2015 ). According to Ojha & Sinha (2017 ), Continuity of care is also a crucial factor for patient satisfaction and it requires partner like relationship between healthcare service provider and patient. However as the changes emerged in healthcare sector for example changes in coverage of health insurance etc may cause a forced discontinuity in patients’ satisfaction. Similarly, the extent to which patients’ are satisfied from a healthcare provider also depends on characteristics of patient and why they are visiting certain hospital for example in serious cases patients may not wait even for one day to see their concerned doctor ( Pakdil & Harwood, 2005 ). Previous researches ( Johansson, Oleni, & Fridlund, 2002 ; Chilgren, 2008 ) also indicated continuity is important in building the trust of patient on some particular hospital. According to Kansra & Jha, (2016 ) there is a strong interaction between continuity and satisfaction and this interaction is complex in nature that involves patients’ characteristics and healthcare factors provided by a specific hospital.
Patient satisfaction is associated with many factors. It may include the waiting time at healthcare center ( Ameryoun et al., 2017 ), physical structure and cleanliness ( Nadiri & Hussain, 2016 ) and responsiveness and assurance ( Khamis & Njau, 2014 ). Furthermore there are many factors that contribute towards patient satisfaction at healthcare centers. It may include the privacy, tangibility, courtesy of staff, clinic environment, registration process and consultation time. The outpatient department (OPD) of any hospital is actually the shop window of any health care centre. Therefore the reaction of patient at OPD reflects the overall satisfaction level of patient for that specific health care unit. Existing literature also advocates that drivers of patient satisfaction vary at public and private health care centers. Even there may be different factors associated with patient satisfaction at developed, developing and least developing countries. It is due to the factor of infrastructure provided by the government to the health care centers. The study is focusing on the factors contributing towards patient satisfaction in developing country i.e. Pakistan.
1.1. Healthcare sector of Pakistan
Pakistan is the 6th largest state of the world but the budget allocated to health is 1.5% of entire budget. Health care sector in Pakistan is running under Ministry of health. There are two sectors public and private. Public sector provides basic health facilities with very low cost whereas private sector charges heavily ( Nishtar, 2009 ). In Pakistan, the infrastructure of health sector is moderate which consists of Rural Dispensaries (RD), Basic Health Units (BHU), Rural Health Centers (RHCs) and the District hospitals. The wide network of health care facilities consists of 4755 Rural dispensaries (RD), 5349 Basic Health Units (BHUs), 572 Rural Health Centers (RHCs), 945 Tehsil and District headquarter hospitals (THQ,DHQ), 903 maternal child health centers (MCHs) and 290 TB Centers (Existing Infrastructure of Health care in Pakistan ( Mushtaq et al., 2011 )
1.2. Problem Statement
Private Healthcare sector is grooming and becoming highly competitive in metropolitan cities of Pakistan like Lahore and Karachi. Healthcare service providers have begun to facilitate their patients with five star treatment facilities ( Ojha & Sinha, 2017 ). Patients of today not only expect state of the art treatment facilities but also other facilities in order to have a pleasant stay at hospital. This adjustment in disposition has come because of commercialization. Presently, delivery of high quality healthcare services is increasing from patient’s side and measurement of satisfaction in patients is very important in this regard ( Al-Borie & Sheikh Damanhouri, 2013 ). This situation stems from the concept of patient satisfaction and quality. So above discussion clearly highlights the importance of present topic, furthermore this study will also investigate the sixth dimension (usability) of SERVQUAL model that was previously investigated in turkey by Strawderman & Koubek, (2008 ).
1.3. Significance and Rationale of the study
Existing literature demonstrates that little work has been done in healthcare sector of Pakistan regarding SERVQUAL model. So this gap provides a good rationale for present study in private healthcare sector of Pakistan. Furthermore it is also evident from existing literature that in developing countries including Pakistan the factor of patient satisfaction is ignored area so it is quite clear that patient satisfaction in developing nations is not given due importance and this is visible in many developing nations. Finally the study will incorporate the sixth dimension usability in SERVQUAL model. The results of present study will help policy makers in framing polices that can improve the standards of healthcare delivery in order to enhance patient satisfaction in private healthcare sector of Pakistan.
2.1. Service quality
“ Peer & Mpinganjira (2012 ) observed that one of the most vibrant factors having an effect on satisfaction is service quality. Considering customer hopes is possibly the most decisive, step in execution of a tremendous service. As detected by “ Slack, Chambers, & Johnston (2010 )”a favorable link exists between service quality and client contentment. Gray (2008 ),” reported as throughout previous twenty years, service quality has turned into a crucial range of consideration towards, directors, executives and intellectuals as of the aforementioned resilient influence upon corporate presentation, profit on investment, customer satisfaction, customer loyalty and achievement of enlarged income. The rapid extension and rivalry of service quality, in both advanced and emerging nations have made it convincing for organizations to judge and calculate the value of service quality“( Brown & Bitner, 2006 )”.
2.2. Healthcare service quality
Gray (2008 ),” described that, with customers of current scenario having a lot of information and experience of the world around them the way to attain advantage in today’s service sector, without negotiation, is through the superiority of service delivered to customers. The health department is not omitted from this perception as there is a growing collection of studies from USA to determine that service quality and patient satisfaction and its direct association to patients’ communicative objectives to re-visit the hospital or applaud it to others.
Patients usually concerned to the service by concentrating on quality “( Solomon, 2014 )”. One more clarification of quality is entire characteristics plus traits of the product or services which depends on capability for contenting specified or concealed desires “( Kotler & Armstrong, 2010 ). This is vibrant as quality is something that may provoke contentment or discontentment of patients. “A diffident definition of quality in health sector is the ability of doing the right thing, at the right time, in the right way, for the right person – and captivating the best feasible outcomes” (Zineldin, 2006 ). Service atmosphere in health sector is decided through not only equipment and innovative facility care, but also work of labor in a hospital. “Abundant methods and tools are applied by health executives, researchers, and healthcare strategy originators in an effort to find a better way to offer great quality of the service” “( Lee, & Kang, 2012 )”.
2.3. Patients vs. Health service providers:
patients’ view of healthcare delivery facility quality might be liable on several features for instance prior knowledge, communal and outmoded duties, health terms, patient demographics (e.g., age, gender), patients’ data for methods and treatment etc “( Sofaer & Firminger, 2005 ). Patients might be embellished by word-of-mouth which involves in erection standing of a healthcare institute ( Chilgren, 2008 ). Recurring to the debate that staff of a hospital plays a key part in achieving high class of health provision. Doctors offer right remedial cure, healthcare directors remain accountable for assuring that deceased persons get proper facilities during treatment at their hospital ( Chilgren, 2008 )”.
Andaleeb, Siddiqui, & Khandakar, (2007 ) determined the factors affecting the patient satisfaction in Bangladesh. They made a comparison of determinants of patient satisfaction on a sample of patients treated at public, private and foreign hospitals. Karekar, Tiwari, & Agrawal, (2015 ) investigated the service quality of hospitals for patient satisfaction by using determinants such as: empathy, tangibles, assurance, timeliness and assurance. They found that service quality at private hospitals was much better as compared to Govt. hospitals. High level of quality of service means more satisfaction. According to the study work of “ Fröjd et al., (2011 )” patients desired to be given extra info and to have capability to contribute in a cure procedure. Thus, this is vital to careful efficient class of service excellence, definitely client-oriented and info measurements.
2.4. Dimensions of Service Quality and Patient Satisfaction
2.4.1. Tangibility and Patient Satisfaction
Tangibility narrates the result of physical facility, apparatus, employees and communication resources for patient. The outcome of these interferences, commonly identified as "services capes" impact patients level of satisfaction in many ways ( Materla, Cudney, & Antony, 2017 ). Brown & Bitner, (2006 ) illuminated how the workers and clients are affected by these tangibles aspects of services in physical, psychosomatic, sociological, intellectual, and passionate ways. According to Kotler & Armstrong, (2010 ) a product goes beyond the tangible features generally connected with it, adding numerous other features, comprising of a scheduled atmosphere, a bundle that establishes the “true product” professed by clients”. The above literature paves the way to state the following hypothesis
H1: tangibility has a positive and significant impact on patient satisfaction in private hospitals of Pakistan.
2.4.2. Reliability and Patient Satisfaction
“Reliability is the ability to produce reliable outcomes ( Kotler & Armstrong, 2010 ). For the client’s overall valuation of service quality, this dimension is very imperative. Hence, organizations should recognize the fundamental prospect of their clients and make accessible the major services in the straightest method ( Goel, 2016 ). Reliability is demarcated as the capability to execute the guaranteed service devotedly and flawlessly ( Cheng Lim & Tang, 2000 ). “ Peer & Mpinganjira (2012 ) observed that among all other service quality components, reliability has repeatedly been shown to be the most important for client satisfaction. On the basis of above discussion, the following hypothesis is developed;
H2: There is positive and significant relationship between reliability and patient satisfaction in private hospitals of Pakistan
2.4.3. Responsiveness and Patient Satisfaction
Societal responsibility is a vital perception, which is possibly neglected absolutely in the quality management writings, however it has repetitively got due respect and demonstration in existing literature ( Goel, 2016 ; Al-Borie & Sheikh Damanhouri, 2013 ). Responsiveness is willingness to offer help and quick services to consumers. This consists of attentiveness and swiftness in dealing with patients wants, complaints and worries. In the hospitals, patients don’t have time to wait for their turn to be entertained. This is the reason that why the waiting time in most hospitals is crucial. The services rendered by the hospitals must be customized to satisfy the single customer’s desire. Every patient in the hospital attains a specific plan of cure because they are suffering from different ailments. Responsiveness means that patients obtain rapid and justifiable care from the hospital workforce as well as being indulged in decisions about their care ( de Jager & du Plooy, 2011 ). According to Peer & Mpinganjira, (2012 ) and Ojha & Sinha, (2017 )” this element stresses thought as well as speed in handling customer queries, objections, requests and troublesomeness. So the following proposition is developed
H3: There is positive relationship between the responsiveness and patient satisfaction in private hospitals of Pakistan.
2.4.4. Assurance and Patient Satisfaction
“Assurance means constantly looking to deliver improved products to clients based on the thought that the uppermost importance is given to quality. A quality assurance structure is supposed to raise customer sureness and an organization's believability, to enhance work processes and proficiency, and to empower an organization to enhanced contest with others. Quality assurance “refers to the procedures, attitudes, activities and processes essential to confirm that quality is being sustained and enriched” ( Kitapci et al., 2014 ; Moore et al., 2016 ). Quality assurance is projected to confirm answerability and/or to bring about enhancement. “Quality occupies the medium ground between the exterior and the interior; a philosophy or structure that emphases and helps the collaboration between the external calls for enlarged answerability and the internal efforts of an institution that is showing it ( Brown & Bitner, 2006 ). Hence it is proposed
H4: There is positive and significant relationship between the assurance and patient satisfaction in private hospitals of Pakistan.
2.4.5. Empathy and Patient Satisfaction
Empathy refers to the visionary forecast into another's emotional state, a state of total identification with another's condition, situation, and opinions. Empathy is the partaking of sensitivity and perspective-taking persuaded by reading, inspecting, hearing, or envisioning descriptions of another’s state and circumstance. Empathy shows a role in the aesthetics of construction when writers experience it ( Peprah & Atarah, 2014 ; Pitt et al., 2016 ). For having a good client relationship, the information of the patients by name is even very significant. In the health department, patients need care. The implication of empathy before and after a treatment builds sureness and trust in the mind of patient. The families of patients stand constantly maddened whereas waiting for the consequence of methods. The family members want gentleness and demand carefulness to decrease the degree of pressure and uneasiness they are going through. Empathy confirms the handling customers as distinctive persons ( Raju & Lonial, 2001 ). So in line with the above discussion the following hypothesis is proposed.
H5: There is positive and significant relationship between the empathy and patient satisfaction in private hospitals of Pakistan.
2.4.6. Usability and patient Satisfaction
Strawderman & Koubek, (2008 ) used human factor in service by including usability factor in SERVQUAL model and the modified model was named as SERVUSE. The frameworks tended to by human factors include apparatuses tools and machines, tasks and jobs, and environments. Apparatuses and machines are things that are used in service procedure. This may incorporate PCs, interfaces, or office accessories. Tasks and jobs are finished all through the service procedure. These might be finished by the client or the organization. Environments are the surroundings of both the client and the organization. They may incorporate an office setting, home, eatery, or even a website ( Sanders & Cormick, 1993 )
Evaluating usability of a system presents many advantages for the client including expanded efficiency, reduced error and time and cost and expanded precision. An organization that makes usable items can profit by more prominent benefits, expanded business and an expansion in client loyalty ( Mayhew, 1999 ). Strawderman & Koubek, (2008 ) found that including usability dimension in SERVQUAL model, delivers a more precise indicator of behavioral intentions of clients. Along these lines, the usability of a framework is an essential player to predict a customer revisit of a healthcare organization. Therefore, the usability of a system is an important factor in predicting a customer’s return behavior. If a system is easy to use, the customer will be more likely to return in the future. If the usability of a system is poor, the customer is likely to become frustrated and not be willing to use the same system in the future. The outcomes of their study strongly supported the inclusion of usability dimension when measuring behavioral intentions. They further recommended that usability ought to be incorporated as an important factor when measuring service quality and patient satisfaction. Hence it is proposed.
H6: There is positive and significant relationship between the usability and patient satisfaction in private hospitals of Pakistan.
3.1. Population and Sample
Simple random sampling approach was adapted as the study focused on a population of in-patients in private healthcare sector of Lahore. To represent private healthcare sector of Lahore three major hospitals, Iqra Hospital, Arif Memorial Hospital and Hameed Lateef Hospital were considered. A self administered questionnaire was distributed among respondents randomly. A total of 348 questionnaires were distributed and a total of 261 fully filled questionnaires were received and hence response rate remained 75 percent.
3.2. Questionnaire
“An adapted questionnaire (Parasuraman, & Grewal, 1988 and Strawderman & Koubek, 2008 ) which featured the 6 dimensions of service quality; tangibility, responsiveness, reliability, assurance, empathy and usability was used to collect the data. Each question in the questionnaire was valued on a five-point Likert scale ranging from 1 for “Strongly Disagree” and 5 for “Strongly Agree”.
“ Table 4. 1 : Gender of Respondents
|
Categories of gender |
Frequency |
Percent |
|||||||||||
|
Male |
171 |
65.5 |
|||||||||||
|
Female |
90 |
34.5 |
|||||||||||
|
Age Limits |
|||||||||||||
|
18-30 |
62 |
23.7 |
|||||||||||
|
31-50 |
108 |
41.4 |
|||||||||||
|
Above 50 |
91 |
34.9 |
|||||||||||
|
Marital Status |
|||||||||||||
|
Single |
62 |
31.8 |
|||||||||||
|
Married |
178 |
68.2 |
|||||||||||
|
Total |
261 |
100.0 |
|||||||||||
The above table presents the descriptive of respondents in term of gender, Age and Marital Status. As it can be seen that majority of respondents were male ( 171) and married (178), similarly the maximum age bracket was 31-50 years of age (108) from a total of 261 respondents.
4.1 Reliability and validity
KMO and Bartlett test was incorporated for checking the appropriateness of scale used in this study and prove about adequacy of sample. Table shows the results for KMO and Bartlett test. The value of KMO is 0.761 which shows more than the appropriateness according to the standard criteria of KMO value 0.50 so KMO value is above average. Bartlett Test is also showing the significant value 0.000 which makes this analysis perfect for performing factor analysis.
Table 2: KMO and Bartlett’s test
KMO measure of sampling adequacy 0.761
Approx. Chi Square 4751.023
Bartlett’s test of sphericity df 426
Sig. 0.000
Gerbing & Anderson, (1988 ) defined various basic guidelines for the reliability and validity of measurement scale used in the study. A step-by-step approach is used for analysis. First of all, it’s necessary to perform factor analysis as data reduction methods in order to lessen the questions in the measurement tool. For the purpose of examining the common variance, all the items were included in the analysis. According to the recommendation of Hair, (2007 ), Promax rotation was used that is an oblique rotation method and set criteria of cut-off value is 0.50 in factor analysis. All the values were above the set criteria of cut-off value. The reliability of this scale was checked with the help of Cronbach’s alpha and set criteria of 0.70. All the variables were having a good reliability of the scale used in this context”.
Table 3: Factor Analysis and Alpha Values
Variables Factors loadings and Cronbach’s
Tangibility 0.799
T1 0.718
T 2 0.808
T3 0.723
T4 0.716
T5 0.854
T6 0.761
T7 0.893
T8 0.726
T9 0.868
Reliability 0.758
R1 0.757 R2 0.894
R3 0.794
R4 0.717
R5 0.734
Responsiveness 0.910
RS1 0.909
RS2 . 0.708
RS3 0.803
RS 4 0.794
RS 5 0.853
RS 6 0.707
RS 7 0.801
RS 8 0.791 Assurance 0.713
AS1 0.725
AS2 . 0.768
AS3 0.861
AS4 0.816
AS5 0.730
Empathy 0.817
E1 0.818
E2 0.791
Usability 0.756
U1 0.763
U2 0.740
U3 0.843
U4 0.772
U5 0.730 Patient Satisfaction 0.950
CS1 0.909
CS2 0.908
CS3 0.803
*Values in bold are Alpha Values
Table 4: Correlation Analysis
|
1 |
2 |
3 |
4 |
5 |
6 |
|
|
Tangibility |
||||||
|
Reliability |
.353** |
|||||
|
Responsiveness |
.257** |
.284** |
||||
|
Assurance |
.341** |
.179** |
.389** |
|||
|
Empathy |
.446** |
.459** |
.306** |
.453** |
||
|
Usability |
.382** |
.273* |
.241** |
.231** |
.193** |
This study used the Pearson correlation in order to check the correlation among different variables. Table 4 shows the confirmation of correlation among different variables in this study. As it can be seen that all predictors are having positive and significant correlation with each other. Similarly the value of correlation among all predictors is modest that is indicative that data is not suffering from multicollinearity issue.
Table 5: Overall Regression Analysis
|
Hypo-thesis |
R Square |
Standard Error |
Beta Value |
T-Value |
P-Value |
Significant/ In-significant |
Collinearity Statistics |
|
|
Tolerance |
VIF |
|||||||
|
H1 |
.473 |
.068 |
0.688 |
16.438 |
.0000** |
Significant |
.691 |
2.74 |
|
H2 |
.599 |
.043 |
0.774 |
21.191 |
.0000** |
Significant |
1.76 |
2.29 |
|
H3 |
.883 |
.021 |
0.940 |
47.710 |
.0000** |
Significant |
1.36 |
1.92 |
|
H4 |
.748 |
.034 |
0.865 |
29.857 |
.0000** |
Significant |
.731 |
1.39 |
|
H5 |
.536 |
.039 |
0.732 |
18.634 |
.0000** |
Significant |
1.12 |
2.21 |
|
H6 |
.586 |
.042 |
0.766 |
20.662 |
.0000** |
Significant |
.935 |
1.39 |
The table represents the results of all the variables which have been observed in the study. All the dimensions of service quality have positive relationship with patient’s satisfaction. In the research, it is found that responsiveness (H3) has the strongest positive relation with patient satisfaction (b=0.883) in private hospitals of Pakistan that means private sector hospitals are providing prompt services to their patients as they approach in a specific private hospital.. Assurance (H4) has the second highest positive relationship with patient satisfaction (b=0.748) meaning that patients have high level of trust and confidence in healthcare delivery services of private sector hospitals. Reliability is third significant factor in present research study (b=0 .599) as mostly patients have shown in present survey that have confidence in private sector hospitals of present study about accuracy in delivering healthcare services. Usability was fourth significant factor contributing towards patient satisfaction of private hospitals (b=0.586) its mean that patients feel ease of learning and memorizing of where, how and from whom to receive the offered healthcare delivery services. similarly, empathy was at fifth place in term of its significant towards patient satisfaction as most of the patients of present study were of the opinion that they receive personalize attention when they visit a specific private sector hospital for any treatment. Finally tangibility factor was at sixth place (b=0.473) but as the beta value is significant so we cannot ignore this factor too because patient of present survey are also keen to observe Appearance of hospital’s facilities, staff, equipment, and communication materials.
The results of present study are evident that usability dimension as the sixth dimension is playing a significant role for enhancing patient satisfaction in private healthcare sector of Pakistan. These results are in line with the findings of Strawderman & Koubek, (2008 ) who also reported that usability as sixth dimension of SERVQUAL model is significant predictor of patient satisfaction in Turkish hospitals.
Similarly all other five dimensions of SERVQUAL model are also predicting patient satisfaction positively and significantly as evident by the results of present study but the responsiveness factor is the most strongest predictor of patient satisfaction in private healthcare sector of Pakistan. This is similar with the findings of Li et al., (2015 ) and Ojha & Sinha, (2017 ) but inconsistent with the findings of Peprah & Atarah, (2014 ) who reported responsiveness dimension is insignificant but his study was in public sector where doctors are not as responsive as it can be observed in private hospitals. So based on the results of present study all hypotheses are producing positive and significant results for private healthcare sector of Pakistan.
Contributions and Implications For Policy Makers
The discoveries of the present investigation are of significance for managers and policy makers of healthcare sector in Pakistan concerning the inpatient part of service quality. The policy makers of healthcare sector must put effort to modernize doctor's facilities and other facilities in order to better satisfy patients satisfaction and level of service quality
In the globalized period, patients have been given a lot of importance because of serious rivalry among the different health service providers. On the off chance that a patient is not happy with the service offered by a specific hospital, he will instantly switch over others hospitals. In this way, top rated hospitals try to give every possible careful consideration in offering patient care services.
In this manner, it turns into a critical to keep up the nature of wellbeing of health services consequently can hold the patients. SERVQUAL strategy for evaluating is generally used to look at the service quality offered by healthcare providing institutions. In this regard the present study is evident that patients of today are very keen in observing how private hospitals are serving them and they think that responsiveness factor of these hospitals is very important as the statistical results of present investigation showed.
There are some important limitations of present study but the author(s) perceive, it opportunity for other researchers to investigate the topic in future by keeping these limitations in mind. The first limitation of study is that it was only focusing on private healthcare sector of Lahore and in private sector three large hospitals were considered so it is suggested for future researchers to investigate the model of present study with a mix of hospital of private and public and similarly hospitals having average ranking and best ranking so that a proper comparison may be drawn. Second limitation of present study is that it only focused on in-patients so future studies can take both in and out patients. Similarly the data was cross- sectional in nature and generizability may be a question as cross- sectional data just provide only one time snapshot and we don’t know any background of the story so future studies need to consider longitudinal data for analysis. Finally the study took into consideration only the functional aspect of SERVQUAL model as it only considered patients’ point of view so for future studies it is suggested that both functional and technical aspects should be considered by taking into consideration the view point of healthcare service providers.
Ahmady, A. E., Pakkhesal, M., Zafarmand, A. H., & Lando, H. A. (2015). Patient satisfaction surveys in dental school clinics: A review and comparison. Journal of dental education, 79 (4), 388-393.
Al-Borie, H. M., & Sheikh Damanhouri, A. M. (2013). Patients' satisfaction of service quality in Saudi hospitals: a SERVQUAL analysis. International Journal of Health Care Quality Assurance, 26 (1), 20-30.
Ali, F., Hussain, K., & Omar, R. (2016). Diagnosing customers experience, emotions and satisfaction in Malaysian resort hotels. European Journal of Tourism Research, 12 , 25.
Ameryoun, A., Najafi, S., Nejati-Zarnaqi, B., Khalilifar, S. O., Ajam, M., & Ansarimoghadam, A. (2017). Factor selection for service quality evaluation: a hospital case study. International Journal of Health Care Quality Assurance, 30 (1).
Andaleeb, S. S., Siddiqui, N., & Khandakar, S. (2007). Patient satisfaction with health services in Bangladesh. Health policy and planning, 22 (4), 263-273.
Brown, S. W., & Bitner, M. J. (2006). Mandating a services revolution for marketing. The Service-Dominant Logic of Marketing: Dialog, Debate, and Directions , 393-405.
Cheng Lim, P., & Tang, N. K. (2000). A study of patients’ expectations and satisfaction in Singapore hospitals. International Journal of Health Care Quality Assurance, 13 (7), 290-299.
Chilgren, A. A. (2008). Managers and the new definition of quality. Journal of Healthcare Management, 53 (4), 221.
Dagger, T. S., Sweeney, J. C., & Johnson, L. W. (2007). A hierarchical model of health service quality: scale development and investigation of an integrated model. Journal of service research, 10 (2), 123-142.
de Jager, J., & du Plooy, T. (2011). Are public hospitals responding to tangible and reliable service-related needs of patients in the new South Africa? Journal of Management Policy and Practice, 12 (2), 103.
Fröjd, C., Swenne, C. L., Rubertsson, C., Gunningberg, L., & Wadensten, B. (2011). Patient information and participation still in need of improvement: evaluation of patients’ perceptions of quality of care. Journal of nursing management, 19 (2), 226-236.
Gerbing, D. W., & Anderson, J. C. (1988). An updated paradigm for scale development incorporating unidimensionality and its assessment. Journal of marketing research , 186-192.
Goel, R. (2016). Measuring patient satisfaction: different strokes for different folks. Paper presented at the 4 th International Conference on Contemporary Marketing Issues ICCMI June 22-24, 2016 Heraklion, Greece.
Gray, B. A. (2008). The influence of service quality perceptions and customer satisfaction on patients' behavioural intentions in the healthcare industry.
Hair, J. F. (2007). Research methods for business.
Johansson, P., Oleni, M., & Fridlund, B. (2002). Patient satisfaction with nursing care in the context of health care: a literature study. Scandinavian journal of caring sciences, 16 (4), 337-344.
Kansra, P., & Jha, A. K. (2016). Measuring service quality in Indian hospitals: an analysis of SERVQUAL model. International Journal of Services and Operations Management, 24 (1), 1-17.
Karekar, P., Tiwari, A., & Agrawal, S. (2015). Comparison of Service Quality between Private and Government Hospitals: Empirical Evidences from Yavatmal City, Maharashtra. International Journal, 3 (6).
Khamis, K., & Njau, B. (2014). Patients’ level of satisfaction on quality of health care at Mwananyamala hospital in Dar es Salaam, Tanzania. BMC health services research, 14 (1), 400.
Kitapci, O., Akdogan, C., & Dortyol, İ. T. (2014). The impact of service quality dimensions on patient satisfaction, repurchase intentions and word-of-mouth communication in the public healthcare industry. Procedia-Social and Behavioral Sciences, 148 , 161-169.
Kotler, P., & Armstrong, G. (2010). Principles of marketing : pearson education.
Lee, S. M., Lee, D., & Kang, C.-Y. (2012). The impact of high-performance work systems in the health-care industry: employee reactions, service quality, customer satisfaction, and customer loyalty. The Service Industries Journal, 32 (1), 17-36.
Li, M., Lowrie, D. B., Huang, C.-Y., Lu, X.-C., Zhu, Y.-C., Wu, X.-H., . . . Chen, S.-Y. (2015). Evaluating patients' perception of service quality at hospitals in nine Chinese cities by use of the ServQual scale. Asian Pacific Journal of Tropical Biomedicine, 5 (6), 497-504.
Madan, M., & Goel, N. (2015). An Empirical study on Assessing Quality of Health care Services offered by private Hospitals Using Servqual model. Paper presented at the XVI Annual Conference Proceedings.
Materla, T., Cudney, E. A., & Antony, J. (2017). The application of Kano model in the healthcare industry: a systematic literature review. Total Quality Management & Business Excellence , 1-22.
Moore, A. D., Hamilton, J. B., Krusel, J. L., Moore, L. G., & Pierre-Louis, B. J. (2016). Patients provide recommendations for improving patient satisfaction. Military medicine, 181 (4), 356-363.
Mushtaq, M. U., Gull, S., Shad, M. A., & Akram, J. (2011). Socio-demographic correlates of the health-seeking behaviours in two districts of Pakistan's Punjab province. JPMA-Journal of the Pakistan Medical Association, 61 (12), 1205.
Nadiri, H., & Hussain, K. (2016). Zone of Tolerance for Healthcare Services: A Diagnostic Model of Public and Private Hospital Service Quality. Argumenta Oeconomica (2 (37)), 245-280.
Nishtar, S. (2009). Choked pipes: reforming Pakistan's mixed health system: JSTOR.
Ojha, V., & Sinha, G. K. (2017). Patient satisfaction using servqual method at a specialty hospital at Ghaziabad. ACADEMICIA: An International Multidisciplinary Research Journal, 7 (2), 10-22.
Pakdil, F., & Harwood, T. N. (2005). Patient satisfaction in a preoperative assessment clinic: an analysis using SERVQUAL dimensions. Total Quality Management & Business Excellence, 16 (1), 15-30.
Panchapakesan, P., Sai, L. P., & Rajendran, C. (2015). Customer Satisfaction in Indian Hospitals: Moderators and Mediators. Quality Management Journal, 22 (1).
Parasuraman, A., Zeithaml, V. A., & Berry, L. L. (1988). Servqual: A multiple-item scale for measuring consumer perc. Journal of retailing, 64 (1), 12.
Peer, M., & Mpinganjira, M. (2012). A gap analysis of service expectations and perceptions in private general practice. African Journal of Business Management, 6 (1), 297.
Peprah, A. A., & Atarah, B. A. (2014). Assessing Patient’s Satisfaction using SERVQUAL Model: A Case of Sunyani Regional Hospital, Ghana. International Journal of Business and Social Research, 4 (2), 133-143.
Pitt, M., Chotipanich, S., Issarasak, S., Mulholland, K., & Panupattanapong, P. (2016). An examination of facility management, customer satisfaction and service relationship in the Bangkok healthcare system. Indoor and Built Environment, 25 (3), 442-458.
Raju, P., & Lonial, S. C. (2001). The impact of quality context and market orientation on organizational performance in a service environment. Journal of Service Research, 4 (2), 140-154.
Sanders, M., & Cormick, J. (1993). Human factors in engineering and design. New York: McHill: Inc.
Slack, N., Chambers, S., & Johnston, R. (2010). Operations management : Pearson education.
Sofaer, S., & Firminger, K. (2005). Patient perceptions of the quality of health services. Annu. Rev. Public Health, 26 , 513-559.
Solomon, M. R. (2014). Consumer behavior: Buying, having, and being (Vol. 10): Prentice Hall Engelwood Cliffs, NJ.
Strawderman, L., & Koubek, R. (2008). Human factors and usability in service quality measurement. Human Factors and Ergonomics in Manufacturing & Service Industries, 18 (4), 454-463.
Yesilada, F., & Direktör, E. (2010). Health care service quality: A comparison of public and private hospitals. African Journal of business management, 4 (6), 962.
Zineldin, M. (2006). The quality of health care and patient satisfaction: an exploratory investigation of the 5Qs model at some Egyptian and Jordanian medical clinics. International Journal of Health Care Quality Assurance, 19 (1), 60-92.

